










Sudden cardiac arrest (SCA) during sports events is a very rare yet commonly fatal complication among athletes and spectators globally, severely impacting teams, communities and sport. Although SCA in athletes is uncommon, it accounts for most sudden deaths in this population, and 80% of cases are completely asymptomatic until onset of SCA.1,2 Regardless of the improved physical fitness of competitive athletes, the incidence of SCA may be greater in athlete populations than in the general population.3,4 Soccer remains the most popular sport in the world, and basketball is one of the fastest-growing sports globally, yet very little is known about SCA in professional soccer and basketball stadiums.5,6 Additionally, spectators, who are individuals in the stadium not in the field of play, have been shown to have a higher risk of SCA than the general population outside of the stadium.3,7 As a result, there is a critical need to focus on prompt SCA identification and immediate treatment, in any professional sports stadium setting.
The most important determinant in SCA survival is time to defibrillation, which outside of a hospital can be done via an automatic external defibrillator (AED).8 Evidence has shown the effectiveness of rapid defibrillation in stadiums and sports clubs globally.3,7,9–11 However, many sports stadiums vary in the presence, location and implementation of AED protocols, possibly leading to a poor emergency response.12,13 Gathering information about this problem could help to identify global solutions to improve AED usage in professional sports stadiums, ultimately leading to improved safety for both athletes and spectators. Therefore, the objectives of this narrative review are to identify the risk factors and global incidence of SCA in professional stadiums, and the implementation of AEDs in this sport setting. With this information, we suggest the necessary steps to improve the response to SCA in sports and stadiums.
Methods
Definition of a Professional Stadium
In this review, we define a professional stadium as a sports stadium or arena used for college-level or professional events. This includes National Collegiate Athletic Association (NCAA) and any equivalent governing body for college athletics involved in soccer and basketball internationally. Stadiums and facilities must have dedicated concourse, stands, staff, spectators and athletes with regular sporting events.
Inclusion and Exclusion Criteria
To be considered for this review, studies had to meet the following inclusion criteria: discussion of SCA in soccer or basketball stadiums, AED use in soccer or basketball stadiums, AED signage, and AED quantity and planning. Papers were excluded if they discussed internal defibrillators, pacemakers and amateur stadiums.
References Retrieval
An electronic search was conducted using Google Scholar and PubMed/MEDLINE databases. Medical Subject Heading (MeSH) terminology was used to determine keywords as follows: ‘AED’, ‘defibrillation’, ‘soccer’, ‘football’, ‘basketball’, ‘stadium’, ‘arena’, ‘sudden cardiac arrest’, ‘sudden cardiac death’, ‘cardiac arrest’, ‘AED signage’, ‘arrhythmia’, ‘fibrillation’ and ‘asystole’.
Results of the literature search were screened based on title and abstract by three investigators (MDB, JMF and AB) with relevant articles being retrieved if reviewers agreed on their relevance. Any disagreements were resolved by consensus.
Results
Incidence of Sudden Cardiac Arrest in Athletes and Non-athletes
SCA is the leading cause of medical death in athletes, however, there is much variation in SCA incidence reporting globally in athletes.1,5,6,14,15 One review reported an SCA incidence for athletes under 35 years old of 2:100,000 athlete-years for college-level athletes, with this current rate being four–fivefold greater than previously estimated in 1995 at approximately 0.33/100,000 athlete-years.16 Other research showed that athletes at all levels of play have an SCA incidence of 0.98/100,000 athlete-years, while athletes between the ages of 14 years and 25 years old have an SCA incidence of 1.91/100,000 athlete-years.17 A recent study found that the risk of SCA in college-aged male athletes is currently 2.85/100,000 person-years and 5.55/100,000 person-years for black male athletes, specifically.15 For soccer, athletes have an SCA incidence of 1–3/100,000 athletes per year in professional soccer athletes and up to 6.8/100,000 athletes per year in young athletes.18,19 In basketball, Harmon et al. found the incidence of SCA to be approximately 9.09/100,000 per year.1
Evidence is conflicting regarding the incidence of SCA in athletes compared with the general population. Although few studies indicate that athletes’ incidence rates of SCA are lower than the general population, most studies indicate that athletes have significantly higher rates of SCA than non-athletes, with ratios being as high as 2.5:1 in athletes compared with non-athletes.4,20–24
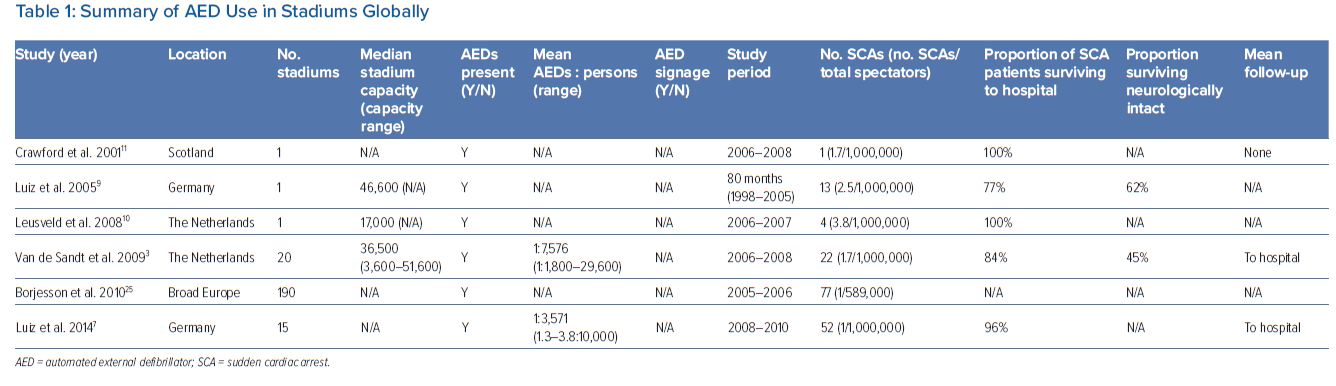
In professional stadiums specifically, the incidence of SCA is larger than in the general population. The spectators’ risk of SCA needs to be considered, in addition to the already mentioned athletes’ risk and incidence. The adjusted incidence is approximately 0.17/100,000 spectators in Europe (Table 1).3,7,25 Comparatively, the incidence of SCA for spectators in Dutch soccer stadiums was nearly fivefold higher than in the general population in the Netherlands, with a stadium-goer incidence of SCA at 0.57/1,000,000 per hour and a general population incidence of 0.11/1,000,000 per hour over the same period.3
Risk of Sudden Cardiac Arrest in Stadiums
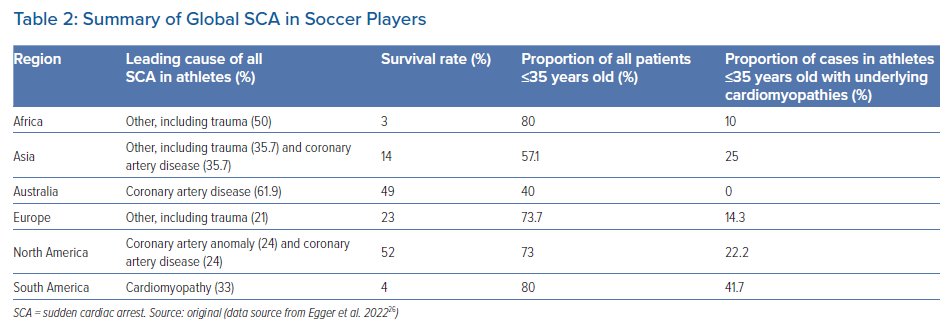
The majority of SCAs in athletes are caused by structural heart disease, such as hypertrophic cardiomyopathy (HCM), bicuspid aortic valves, dilated cardiomyopathy and arrhythmogenic right ventricular cardiomyopathy, primarily presenting with VF, pulseless ventricular tachycardia (VT), asystole and pulseless electrical activity.5,15,16,23,26,27 Recent research has found conflicting evidence stating that most young individuals who die from SCA have a structurally normal heart, however, autopsy reports were unable to be retrieved for 18% of these cases in one study.16,14 Unique to South America is that the leading cause of SCA in young Hispanic athletes under 35 years of age is underlying HCM, while simultaneously having the largest proportion of SCA cases in athletes under 35 years old alongside Africa (Table 2).26
Elevated physical strain of high-intensity activity may act as a trigger for SCA, possibly explaining why SCA primarily occurs during training or within 1 hour following training.5,6,14,21,28–30 In fact, all cases of SCA from 1999 to 2005 in an intercollegiate cohort occurred during some form of physical activity or training.31 Physical activity may increase the risk of SCA by increasing adrenergic tone, which may itself trigger a fatal arrhythmia such as VF in different clinical settings such as an acute MI, long QT syndrome or HCM.32,33
The subgroups at higher risk for SCA globally include black, male athletes in soccer and basketball, with the risk of SCA being significantly higher in these cohorts compared with female and non-black athletes.15–17,22,24,29,34–37 In fact, SCA in women participating in competitive or recreational sport activities was 30-fold less prevalent than in men, indicating a significantly reduced risk in female sport participants.38 Additionally, younger athletes have a greater risk of SCA than athletes at all levels of play.17
It is important to highlight that, while athletes are at risk for SCA in stadiums, there is also an elevated risk of SCA in spectators as well.3,7 Risk factors for them include spectators’ demographics, physical and emotional stress, substance abuse and meteorological conditions such as high heat and humidity.3 Additionally, individuals who experience SCA in stadiums are significantly less likely to have underlying cardiac disease than individuals experiencing SCA outside of stadiums.39 Moreover, the risk of SCA is more than doubled in the surrounding areas of the home arena during match day.40 Likewise, the incidence of SCA has been found to increase in stadiums when the home team is playing a ‘notable rival’ team, possibly caused by emotional stress and substance abuse prior to the match.11 SCA is not limited to spectators or athletes, however, given that 16.5% of casualties in a Glasgow soccer stadium’s survey were from non-spectators, including staff.11
Therefore, compared with the general population, stadiums require focused investigation and caution to ensure that this increased incidence and risk of SCA is monitored closely and treated effectively to prevent undesirable consequences.
Regional Trends of Sudden Cardiac Arrest in Soccer and Basketball
There are many variations in the outcomes and aetiologies of SCA internationally. In a cohort spanning 4 years in the US, the fatality rate was over 50% for SCA in youth athletes, while the SCA fatality rate for mostly European youth athletes remained above 96%.5,35 In a large registry conducted by FIFA between 2014 and 2018, 617 cases of SCA in soccer players were identified from 67 countries. Of these 617 cases, survival was noted in 142, producing a global average survival rate of 23%.26 North America and Australia had the highest survival rates, while Africa and South America were found to have the poorest outcomes (Table 2).26
In the US and Japan, basketball is the sport in which the most cases of SCA occur in college sports, with an annual death rate of 1:11,394 in the US.5,29,36 There is a considerable lack of information about SCA in basketball in most of Asia, Africa, Europe, Latin America and Australia.41
Effect of AED on Sudden Cardiac Arrest Outcomes
It is recommended that AEDs must be implemented in every scenario of SCA.25,42,43 The survival rate of a patient with SCA decreases by 7–10% per minute until defibrillation is delivered.12,44,45 Therefore, the most important determinant for survival in shockable SCA is a deliverable shock from a defibrillator within 3–5 minutes after onset of arrest.45
Many sports programmes and stadiums require prophylactic cardiac screening to possibly identify an individual with an underlying risk factor or condition. However, the risk of SCA remains elevated in athletes despite the implementation of cardiac screening due to the presence of false-negative ECG screens, hidden structural cardiomyopathies, ion channel disorders, commotio cordis and acute myocarditis, among others.46,47 This further supports the on-site placement of AEDs in stadiums.
Cardiopulmonary resuscitation (CPR) is critical to the survival of patients undergoing SCA. In global registries of SCA in soccer players, prompt CPR increased the survival rate to 50% from the global average of 23%.26 However, survival is significantly improved when CPR is used in conjunction with an AED compared with CPR alone.12,26,44,48 There are in fact significantly improved survival outcomes in stadiums because of greater availability and faster response of AEDs in these places than in the local community and emergency medical systems (EMS).26 In one Swedish cohort from 2011 to 2014, the survival after SCA in stadiums was significantly higher than in the public, with a 30-day survival rate of 55.7% compared with 30.4%.49 Similar findings were seen in France from 2005 to 2010, where the survival of SCA in stadiums was 22.8% while public survival after SCA outside of stadiums was 8.0%.39
In athletes, conflicting evidence arises from AED implementation in SCA in stadiums. Historically, college athletes have been found to have poor SCA survival despite defibrillation.50–52 However, international registries and recent data suggest improvements in young athletes facing SCA when treated with an AED, with an increase in survival to up to 85%.26,53 Data reported not from stadiums specifically, showed that AEDs have been markedly effective at improving survival through bystander implementation in public spaces. Hallstrom et al. showed that training bystanders to use AEDs with CPR compared with CPR alone led to significantly improved survival in SCA without any inappropriate shocks.54 Furthermore, public AED use combined with CPR in SCA cases in athletes aged 18–35 years led to a survival greater than 90%, according to a recent prospective cohort study. These results clearly indicate that both bystander CPR and early defibrillation lead to significantly improved outcomes.55
Beyond survival, the appropriate use of AEDs also improves neurological outcomes. In two European soccer stadiums, on-site defibrillation of SCA resulted in survival with positive neurological outcomes in up to 62% of cases (Table 1).3,9 Additionally, public AED use doubles neurologically intact survival compared with AEDs provided through dispatched EMS largely due to a reduction in time-to-shock improvement, which may suggest that spectator use of AEDs can assist in survival in stadiums.56 Similarly, in college athletes, AED use by an athletics trainer on site was significantly shorter than relying on EMS, reducing the average time of defibrillation from 5.2 to 1.6 minutes.31
Sufficient AED Quantity and Location
Despite the evidence that AED use significantly improves SCA outcomes, many stadiums do not have on-site AEDs. Less than 50% of Canadian university sports programmes reported bringing an AED on-site for field sports.57 A broad investigation of the status of professional soccer stadiums across Europe indicated that only 72% of stadiums across Europe did have AEDs present for matches and training sessions, with 74% reporting that there was no advanced CPR training available.25 However, disparities exist between countries in more recent individual studies. For example, English professional soccer stadiums now have AEDs at all training and match days.58 Despite this individual study, there is a lack of more recent information for Europe. In a cross-sectional study of 16 sports centres in Italy, 48.4% of stadium staff claimed to not know whether there was an AED in their stadium, 38.1% were unsure where the AED was placed, and nearly 80% admitted to not having any medical training with limited knowledge of AED use.59 Many stadiums that did not have AEDs on site relied on local EMS or community defibrillation in response to SCA, although the EMS response often took more than 10 minutes to transport the patient to the nearest hospital in 33% of all stadiums.25
To identify the appropriate location and quantity of AEDs, the American Heart Association recommends an AED no more than 1–1.5 minutes away or approximately 160 m from where a crisis may occur.60 The minimum number of AEDs for this desired response can be calculated using a function of estimated time needed to traverse the longest distance in an arena, slope and possible worst-case scenarios.61 In addition to this calculation, medical professionals can estimate the number of AEDs required for mass gatherings by using a separate function of stairway slope in the stadium, stadium congestion and the time required to cross a horizontal distance to calculate the required number of AEDs.62 This alternative function considers the time required for a first responder to grab the defibrillator, unpack it, and place electrodes on the patient, giving a more accurate estimate of the response time.
There are many factors that act as facilitators or barriers that influence AED implementation. The most significant predictors of college sport departmental AED ownership are unit cost, donated units, and proven medical benefit, with the most frequent predictors of AED ownership being proven medical benefit, concern for liability, and affordability.63 Focusing on these factors will improve the odds of athletic departments and stadiums owning and maintaining AEDs on site.
AED Signage
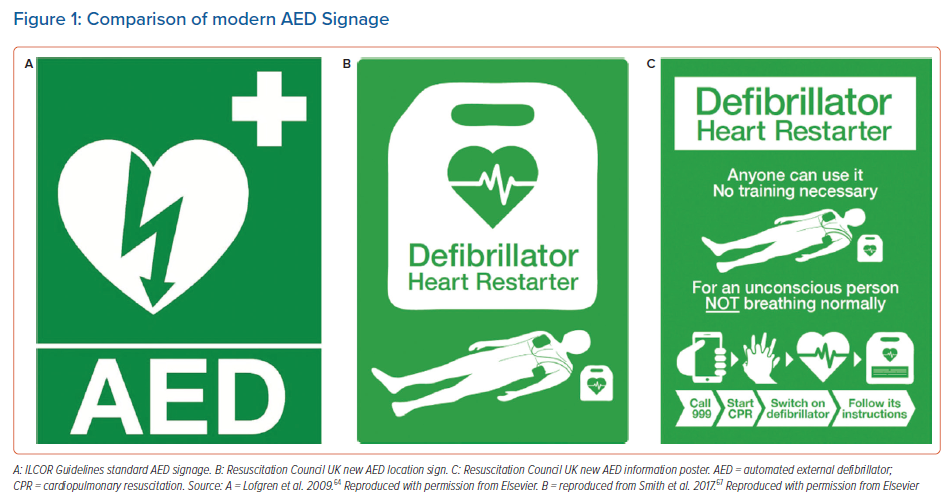
Adequate signage for the location of an AED is a critical component of all out-of-hospital SCA response programmes. The most common signage standard is the International Liaison Committee on Resuscitation (ILCOR) guideline used internationally (Figure 1A).64 However, this often has poor recognition by public bystanders. Travellers from 42 countries were able to correctly identify the ILCOR AED sign only 39% of the time, with other research showing a range of recognition from 29.4% to 47.9%.65–67 Furthermore, 26% of Dutch medical professionals were unable to recognise an AED when pointed directly to one.68 First responders are aware of an AED present only in 4.25% of SCAs outside of a hospital.69 In response to these poor outcomes, the Resuscitation Council of the UK compiled more modern imaging and instruction guidelines for AEDs that 83.5% of the public agreed on (Figures 1B and 1C).67
Adequate signage status varies and may be hard to identify given the critical absence of reliable public data. Currently, most UK public AEDs do not have any signage at all, with only 2.5% having accessory signage more than 5 metres away to guide first responders to its location.70 Finally, more than 40% of all public UK AEDs with signage were at least partially obstructed, with more than one-third having no external lighting, making them more difficult to find in darker settings.70 Although these data do not originate from stadiums, the fact that individuals and healthcare professionals are unable to adequately identify and retrieve AEDs in public due to poor signalling is important to highlight. In a stadium setting, relying on fast responses is critical in the SCA response, and both bystanders and the stadium medical staff must be able to quickly find and use the AED, thus highlighting the need for improved signalling that is paralleled in the public setting from these studies.
Role of the AED in an Emergency Action Plan
One of the most important factors in administering rapid defibrillation is the development and implementation of an emergency action plan (EAP), which many stadiums lack given that only 82% of stadiums in England have a recorded EAP.58 Siebert and Drezner recommend a 7-step plan for a stadium’s EAP for directing medical staff in the event of SCA.42 This plan requires mandatory AED and CPR training for personnel, strategic AED placement and signage specific to the stadium, reliable communication strategies between staff and EMS, immediate AED access, regular review and routine practice, cooperation with an advanced cardiac care facility, and replacement of AEDs after usage with debriefing and reporting.42 For mass gatherings of >1,000 people, such as in stadiums, it is recommended that AEDs act as the foundation in the EAP for medical care.71 It is strongly encouraged that the EAP is written down and that AEDs are registered with the local EMS.8 All personnel should be trained and certified in cardiovascular emergency care, including staff, physiotherapists and athletics trainers to recognise the signs of SCA in order to quickly implement CPR and an AED.42,72,73 A local licensed physician is also recommended to act as medical director, who is familiar with local medical resources and triage decisions to assist in improving the SCA response and updating the EAP regularly in response to new data, research and debriefing for the team.74 However, more than 50% of basketball coaches and staff claim that they have no affiliated medical director or athletics trainer, highlighting an area of possible improvement in these sports and stadiums.75
AED Regulation and Laws
Legal requirements for AED placement differ internationally and may hinder SCA response. In the US, only 15 states legally require AEDs to be placed on-site in health, fitness and/or athletics facilities.76 Although all EU member nations fall under the European Medical Device Directive ensuring standardisation across medical devices used, such as AEDs, there is currently no legal obligation enacted by the EU mandating public AEDs. Many countries, however, have enacted national legislation regarding AED implementation in public spaces, such as France, which requires all public access buildings, including stadiums, to have an AED.77
Results from the most recent survey across European countries showed that 15 countries have laws allowing citizens to use AEDs without a training licence, while three countries require it.78 Specifically, Russia alone requires AEDs to be used only by EMS providers, not bystanders, something that has shown poor outcomes in out-of-hospital SCA response globally.12,56,78
Like Europe, Latin American nations differ in their regulations for AED use in stadiums. Colombia recently decreed AEDs mandatory in places where a mass audience congregates, such as stadiums, joining other Latin American nations such as Puerto Rico, Uruguay, Chile and Argentina.79 Many Asian nations have regulations, such as Malaysia, which recently mandated that public facilities such as stadiums will require an AED by 2025.80 Australia recently enacted mandatory AED placement in public spaces, including sports centres and stadiums.81
Worldwide legal variation across regions and the lack of mandatory placement in public spaces across nations is likely to have worsened the response to SCA. Focusing on reducing this variation, improving access, and allowing bystanders to use AEDs legally may save lives in stadiums.
Discussion
It is evident that SCA should be a critical focus for athletes and spectators in stadiums. Given that HCM and electrical disorders are the leading causes of SCA in athletes under 35 years of age internationally, CPR alone may not be an effective mechanism of resuscitation as compared with CPR with an AED.5,12,15,23,26,27,44,82 Regardless, it is recommended that athletes and coaches themselves learn basic CPR training given that the majority of first responders to SCA were players themselves on the pitch.8,26 Additionally, medical training should be incorporated into routine practices of the EAP.42,74 Regardless of the risk factors or causes of SCA, it is critical to highlight the exceptionally high fatality rate of SCA in stadium-goers that requires intervention with AEDs as a mainstay of treatment.
In global trends of SCA, South America and Africa appeared to have the worst survival rates globally.26 Hispanic athletes have the largest proportion of cardiomyopathies such as HCM in athletes under 35 years old, suggesting that South America may particularly benefit from increased AED availability.26 Due to poor outcomes, aetiologies and lack of available data, future research should focus on Latin American and African outcomes and AED implementation.
There is a key lack of information on the global incidences of SCA in basketball outside of the US and Japan. Hence, a focus on investigating regional differences will enable better planning and adequate implementation of necessary regulations and tools to combat SCA, including possible registries to better track SCA cause, incidence and outcome in these regions in sport and in public.
Given that many stadiums globally rely on local EMS for defibrillation rather than the acquisition of on-site AEDs, this often surpasses the 3–5-minute target for defibrillation.12,26 This further suggests that having widespread AED and CPR available for on-site defibrillation will improve outcomes in stadiums. Although overall survival is immensely important and often the primary outcome, quality of life following an SCA is severely affected by diminishments in neurological function that may have been prevented with AED use and is something that should be considered.
More research investigating stadium SCA incidence, survival and AED implementation to find the optimal AED:capacity ratio may assist future guidelines and regulations for AED requirements. Focusing on the factors that facilitate AED ownership and AED signalling is critical in improving AED implementation, given that identifying factors that improve ease of access in stadiums will save lives. AED signage must be more consistent with modern standards so that in a highly congested and busy area, such as a full stadium, first responders can retrieve them efficiently.
Our recommendations are in line with multiple reviews and consensus guidelines on how stadiums and athletics programmes should respond to SCA.8,24,74,75,82 Here, we outline and summarise the risks of SCA in stadiums globally and the need for AED implementation, maintenance and routine practices involving AED use on-site through an EAP.
Limitations
Limitations include heterogeneous findings across multiple results, including incidences and risk factors for SCA and a lack of information regarding basketball SCA aetiologies and trends globally. Additionally, most of our results originated from North America and Europe, limiting the global implications of our results. Finally, many articles investigating SCA in soccer and basketball stadiums are unclear in follow-up, survival and number of AEDs present, restricting the ability to recommend an optimum number of AEDs from current research alone.
Conclusion
SCA is a highly fatal occurrence in stadiums. Young, black, male athletes in soccer and basketball are at the highest risk of SCA and, currently, many settings have negative outcomes due to poor defibrillation implementation. CPR in conjunction with on-site AED use, continuous training and appropriate signage are a critical part of the EAP of a stadium to improve survival, however, many stadiums worldwide must adopt modern standards to appropriately respond to SCA.
Clinical Perspective
- Stadiums have elevated incidences of sudden cardiac arrest (SCA) for athletes, spectators and staff. Therefore, automatic external defibrillators (AEDs) should be in sufficient quantity and located strategically in response to SCA in the concourse and stands.
- Young, male, black athletes are at the highest risk of SCA in sport. Soccer and basketball are commonly the sports with the highest incidences of SCA. While screening programmes exist for these athletes and sports, many causes could go undetected and thus should not exclude having an AED on-site.
- SCA survival and positive neurological outcomes significantly improve when an AED is applied on site, rather than waiting for emergency medical systems (EMS). Given that many stadiums rely on EMS or local AEDs more than 10 minutes away, stadiums should invest in acquiring, maintaining and training for AED use on-site.
- Adequate visibility and signage improve the ease of use and rapidness of AED application. The use of clearly visible consistent signage, with bright colours, instructions and additional directional signage >5 m away will enable faster delivery of defibrillation.
- Each professional stadium and sports programme should have dedicated medical staff and an emergency action plan prepared to respond to an SCA in the stadium, in which the plan must be practised at least once per year to improve, review and revise the response to SCA.